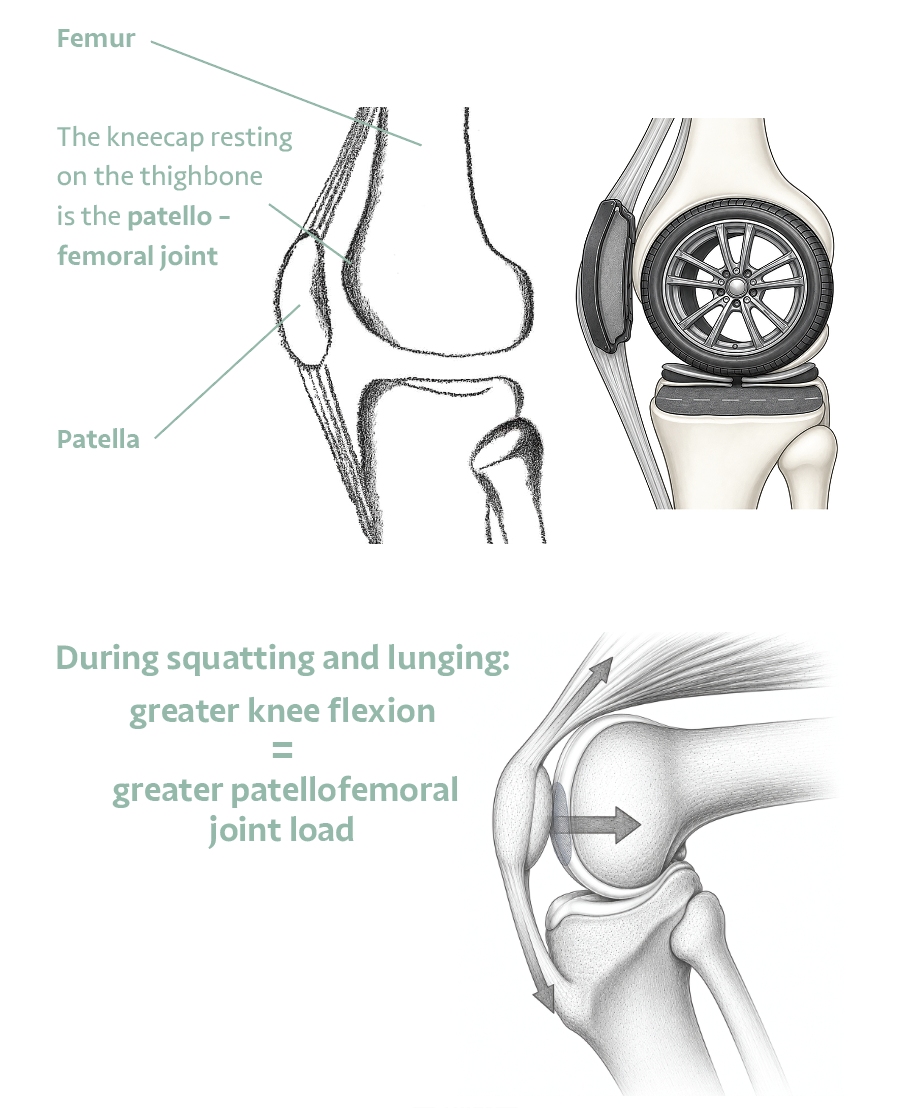
The patella rests in a groove on the femur. This joint transmits enormous forces during everyday activities and is one of the most common sources of knee pain — especially in active people.
HOW IT WORKS
The Patellofemoral Joint Under Load
The patellofemoral joint is formed where the kneecap meets the groove on the front of the thigh bone. As the knee bends, the patella tracks through this groove, guided by the balance of muscle forces around it — primarily the quadriceps and the structures on either side of the kneecap.
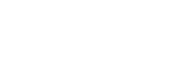
The load through this joint increases significantly with knee flexion. Walking generates approximately half body weight across the patellofemoral joint. Climbing stairs generates roughly three times body weight. A deep squat can generate forces of six to eight times body weight.
Pain in this joint often reflects how it is being loaded, not permanent damage. Muscle imbalance, repetitive impact, and previous injury are common contributing factors.
STAT HIGHLIGHTS
- 0.5x — Body weight — walking
- 3x — Body weight — stairs
- 6–8x — Body weight — deep squat
‘Stand up slowly and evenly from a chair. Notice how the kneecap feels. This small act reveals a great deal about your patellofemoral joint.’
COMMON CAUSES OF PAIN
Why the Patellofemoral Joint Becomes Painful
COMMON CAUSES
- Muscle imbalance — particularly weak VMO (inner quad)
- Tight lateral structures pulling the patella off-track
- Sudden increase in training load
- Previous injury or surgery
- Anatomical factors — groove depth, kneecap height, alignment
MANAGEMENT
- Quadriceps strengthening — especially VMO
- Hip and glute strengthening
- Activity modification — reduce high-flexion loading
- Taping or bracing for symptom relief
- Gradual return to sport with load management