The menisci are two crescent-shaped structures between the femur and tibia. They distribute load, absorb shock, and protect the bone surfaces. Not all tears need surgery — and understanding the type and context of a tear is essential to making the right decision.
ANATOMY
What is the Meniscus?
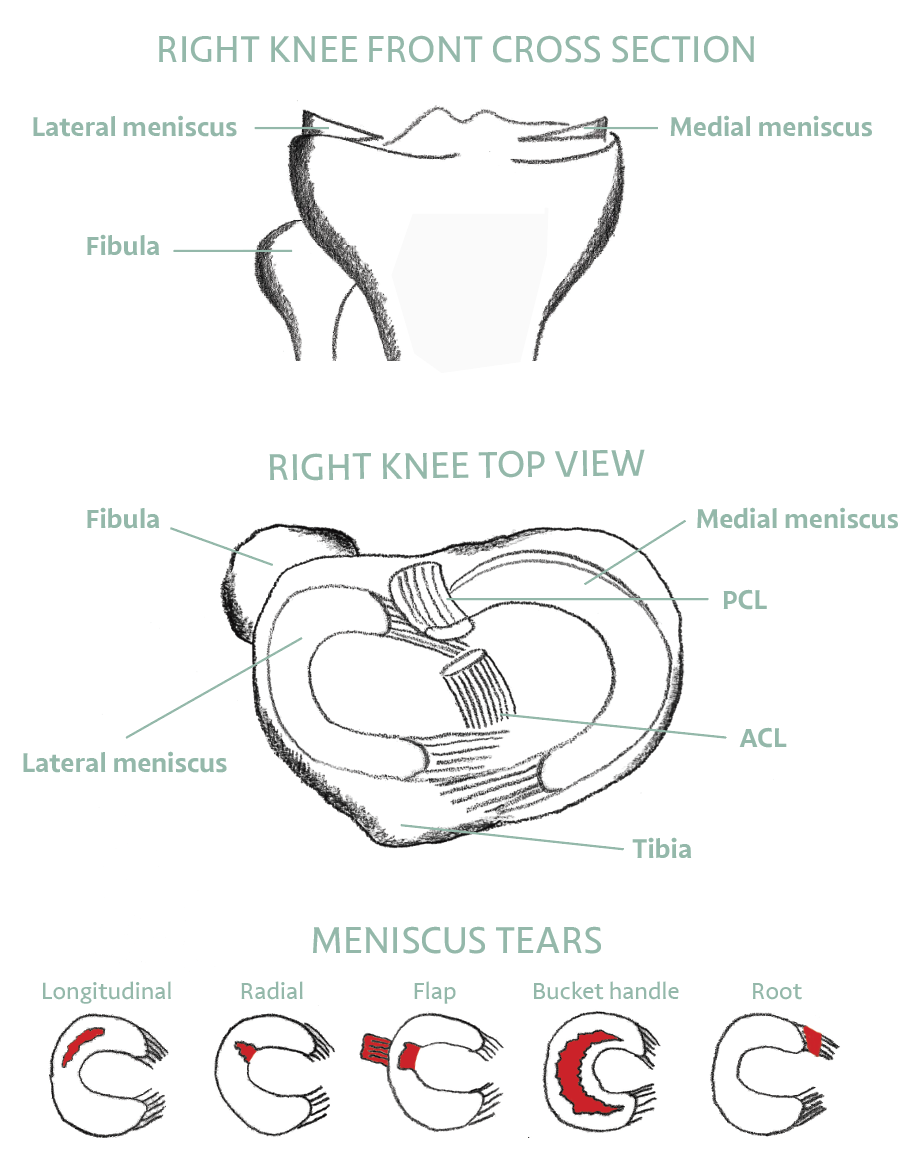
The meniscal cartilages are C-shaped structures that sit between the femur and tibia, helping reduce pressure between the bones and absorbing shock during weight-bearing. There are two menisci in each knee: the medial meniscus on the inner side, and the lateral meniscus on the outer side.
The meniscus is one form of cartilage — known as fibrocartilage, made primarily of Type I collagen. This should be distinguished from the shiny hyaline cartilage (Type II collagen) that lines the bone surfaces and allows low-friction movement. Both are important; both are served by regular movement.
The menisci transmit 50 to 70 percent of load across the knee in extension and up to 85 percent in flexion. They also contribute to joint stability, lubrication, and proprioception — the body’s sense of joint position.
‘When you pivot, turn smoothly and with control. Squat and lunge with good form. The meniscus is stressed most by sudden twisting and deep, uncontrolled bending.’
HOW TEARS HAPPEN
Causes of Meniscal Tears
Meniscal tears occur in two main ways. In younger patients, tears usually involve a significant injury — often twisting and impact — and may be associated with damage to other structures such as the cruciate ligaments. The tear is typically noticed at the time of injury.
In older patients, a gradual weakening and thinning of the meniscal tissue can occur with age, or can be associated with chronic conditions such as diabetes or hypothyroidism. This degenerative process can lead to a small, progressive tear that may not be noticed at the time it develops.
SYMPTOMS
How Do I Know if I Have a Meniscal Tear?
DIAGNOSIS
How is a Meniscal Tear Diagnosed?
Most tears are suspected based on clinical history and examination. An MRI scan is the most reliable way to confirm the diagnosis and characterise the tear — its type, location, and whether it has displaced. X-ray alone cannot diagnose a meniscal tear as the meniscus is soft tissue, not bone.
Movement quality often matters as much as the MRI report. Many people over 40 have degenerative meniscal changes on MRI with no pain at all. The scan must always be interpreted alongside symptoms and clinical examination.