Chondral cartilage covers the bone surfaces of the knee, allowing near-frictionless movement lubricated by synovial fluid. When it is damaged — through injury, repetitive stress, or a condition called osteochondritis dissecans — the consequences range from persistent pain to early arthritis. Understanding the type and stage of injury is essential to choosing the right treatment.
THE GLIDE LAYER
What Chondral Cartilage Is
Articular (hyaline) cartilage is the smooth, glassy tissue covering the ends of the femur, tibia, and the back of the patella. It is between 2 and 4 mm thick and has a coefficient of friction lower than ice on ice. The knee joint produces synovial fluid which both lubricates and nourishes this cartilage — since cartilage has no blood supply of its own, it depends on movement to circulate nutrients.
The chondral cartilage is not to be confused with the meniscus cartilage. The meniscus is fibrocartilage (Type I collagen) acting as a shock absorber between the bones. Chondral or articular cartilage is hyaline cartilage (Type II collagen) acting as the frictionless glide surface on the bone ends. Both types are important; both require protection.
Cartilage does not regenerate easily once damaged. This makes protecting and nourishing it through lifestyle, appropriate exercise, and timely treatment especially important.
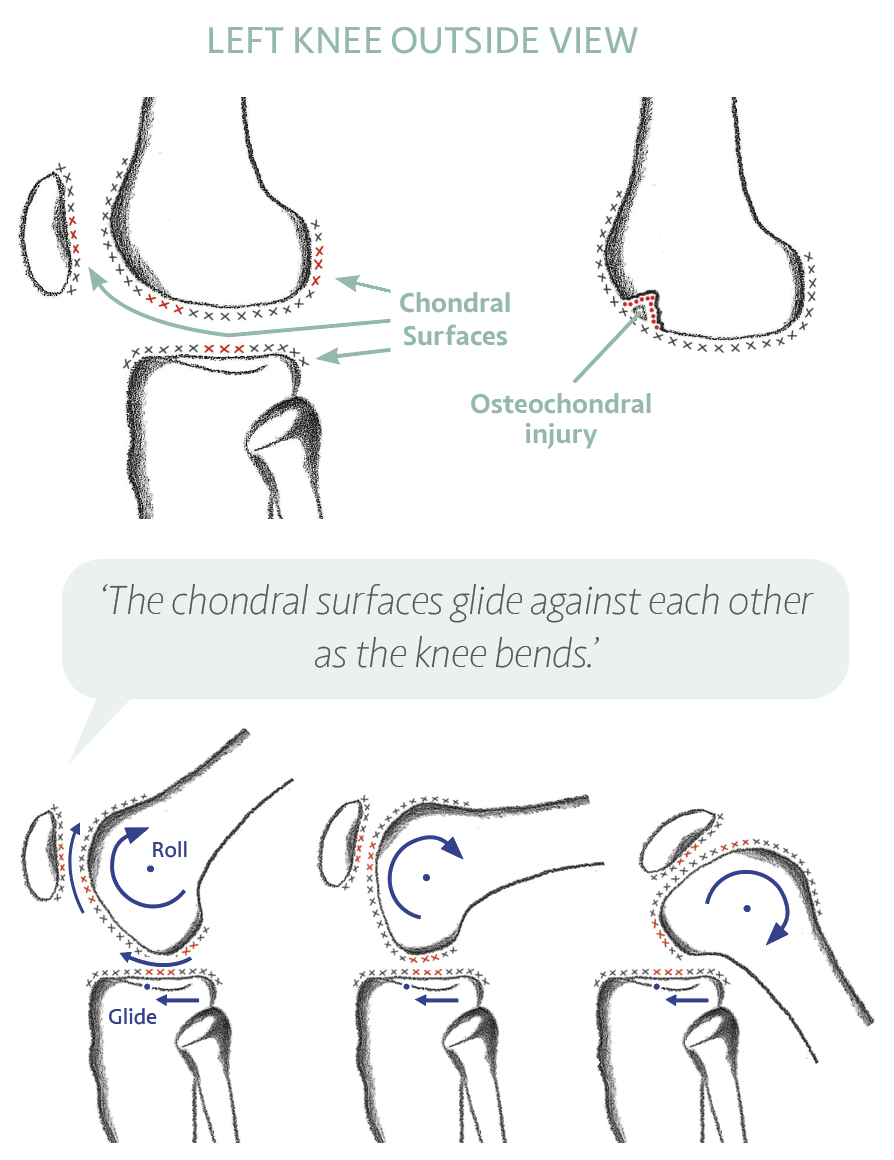
‘Meniscus is one type of cartilage. Chondral is another. Regular, gentle movement nourishes both — it circulates the synovial fluid that feeds the cartilage.’
ACUTE INJURY
Osteochondral Injury and Fracture
An osteochondral injury involves damage to both the chondral cartilage surface and the underlying bone. It can occur as a result of a traumatic injury — such as a direct blow, a fall, or the force generated during a knee dislocation — or from repetitive mechanical stress over time.
The symptoms of an osteochondral injury include pain, swelling, stiffness, a sensation of clicking or catching in the joint, and in more severe cases, locking or giving way. These latter symptoms may indicate that a fragment has become loose within the joint.
MRI scan is the most reliable test for confirming and characterising the injury. It shows the size, depth, location, and whether the fragment is stable or at risk of loosening.
NON-OPERATIVE TREATMENT
- Rest from impact activities
- Physiotherapy — strength and range of movement
- Protected weight-bearing if advised
- Repeat MRI at 3 to 9 months to confirm healing
- Healing can take 6 to 12 months in milder cases
WHEN SURGERY MAY BE NEEDED
- Fragment loose in the joint (catching or locking)
- Defect not healing after 6 months of rest
- Full-thickness defect with fluid beneath on MRI
- Lesion in a young, active patient at risk of early arthritis
- Large defect or one in a high-load area
Surgical options depend on the size, location, and condition of the defect. Most procedures are performed arthroscopically (keyhole), though large defects or those at the kneecap may require a small open incision of 3 to 5 cm.