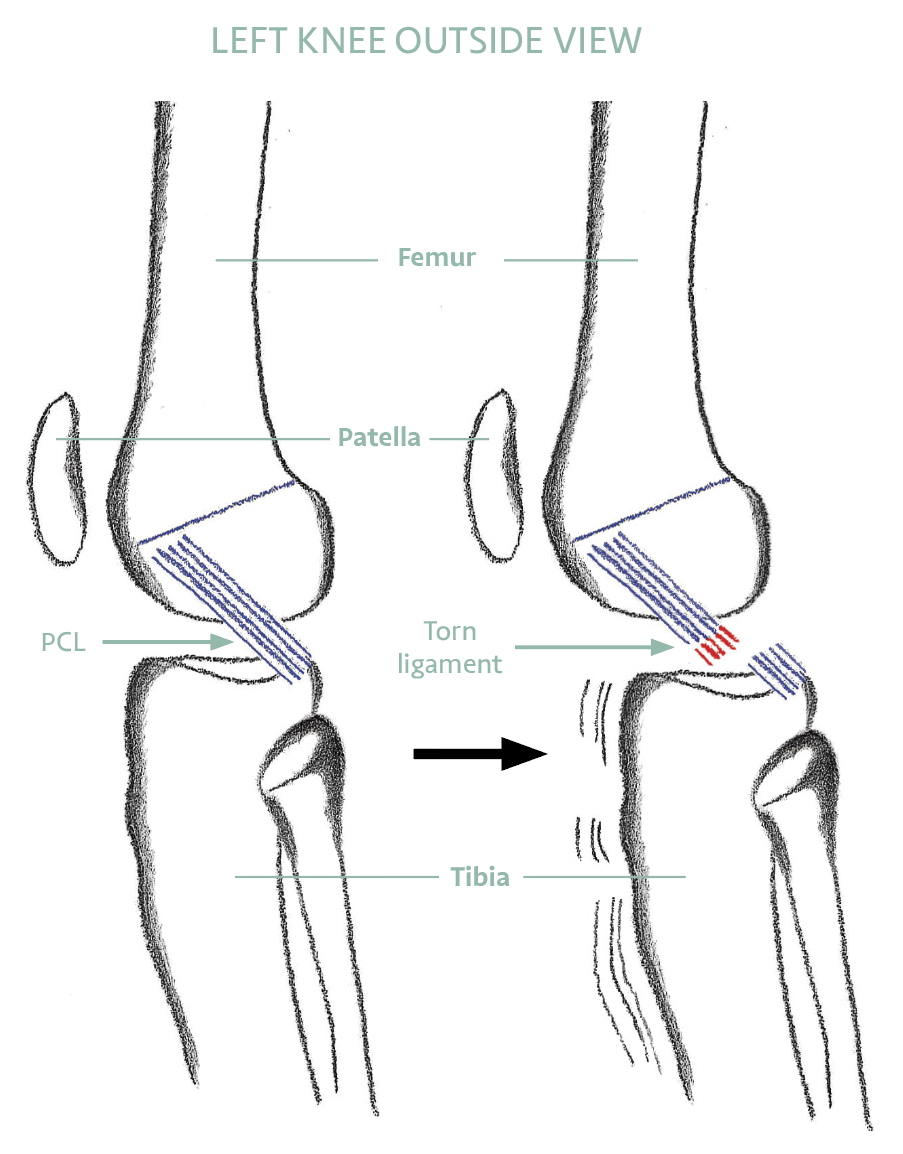
The PCL prevents the tibia moving too far backwards. It is the strongest ligament in the knee and often heals well without surgery. A PCL-injured knee can become strong, stable, and reliable with the right rehabilitation programme.
ANATOMY AND FUNCTION
What the PCL Does
The PCL is the primary restraint against the tibia sliding backwards relative to the femur. It is approximately twice as strong as the ACL and has a better blood supply, which contributes to its superior capacity to heal without surgical intervention.
PCL injuries typically occur from a direct blow to the front of a bent knee — a dashboard injury in a car accident, a fall onto a bent knee with the foot plantar-flexed, or a direct tackle in sport. They can also occur with severe hyperextension.
Isolated PCL injuries often go undiagnosed because the initial swelling is less dramatic than an ACL injury. A posterior sag of the tibia — visible when the knee is bent at 90 degrees — is the classic clinical sign.
HOW IT WORKS WITH OTHERS
More Than One Job — and Rarely Alone
Preventing the shin from sliding backwards is the PCL’s main job, but it is not its only one. The PCL also provides quieter, secondary restraint against the knee twisting outwards and against side-to-side opening — particularly when the knee is close to straight. In the language clinicians use, it is the primary restraint to backward movement and a secondary restraint in several other directions: a genuine multi-tasker.
Just as important, the PCL rarely acts alone. The task of resisting backward movement is shared with neighbouring structures, including the meniscofemoral ligaments described in the research below, and the PCL works closely with the posterolateral corner on the outer back of the knee (Destination 9). When the PCL and the posterolateral corner are injured together, backward and rotational looseness increases far more than with a PCL injury alone. That is why a thorough assessment never stops at the PCL — it always checks the corner too, because getting the whole picture right is what makes rehabilitation succeed.