DIAGNOSIS
How is an ACL Injury Diagnosed?
TREATMENT OPTIONS
Rehabilitation or Surgery
After an ACL injury, some people benefit from reconstruction while others recover well through rehabilitation alone. The decision depends on age, activity level, the degree of knee instability, and whether other structures were injured. It should be made together with your surgeon based on your specific circumstances.
REHABILITATION ROUTE
- Appropriate for many patients — particularly lower pivoting demands
- Excellent outcomes with a structured programme
- Avoids surgical risks and recovery period
- Can always proceed to surgery later if instability persists
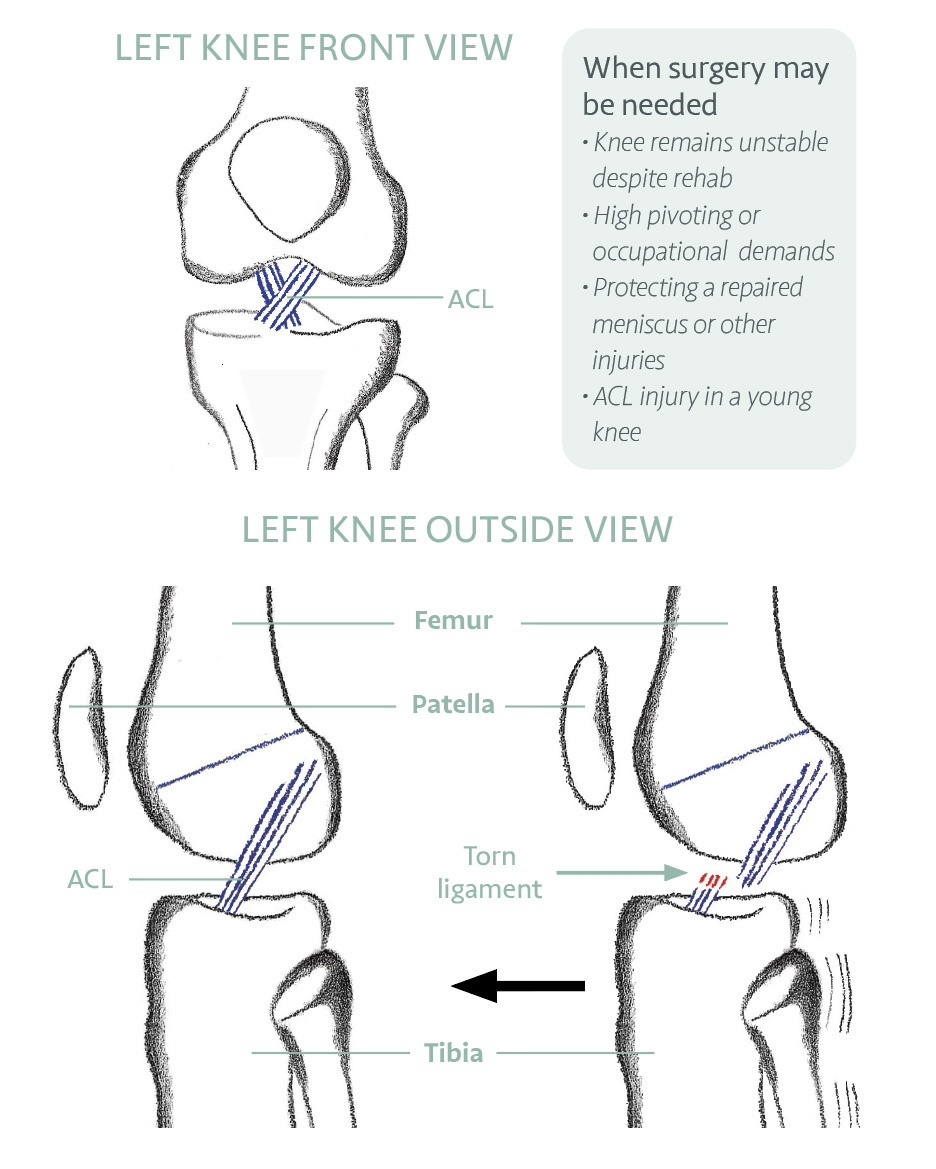
WHEN SURGERY MAY BE NEEDED
- Persistent instability despite thorough rehabilitation
- High pivoting or occupational demands
- To protect a repaired meniscus or other injured structures
- ACL injury in a young, active knee
SURGERY
ACL Reconstruction — What is Involved?
ACL reconstruction involves replacing the torn ligament with a piece of tendon (graft) from elsewhere, usually from the same knee. The most commonly used grafts are from the hamstring tendon, patellar tendon, or quadriceps tendon. A cadaveric (donor) graft is also an option in certain cases. Mr Gupté will discuss the most suitable choice based on your anatomy, age, and goals.
The procedure is performed arthroscopically (keyhole surgery). Bone tunnels are drilled into the femur and tibia to position the graft, which is then secured with screws and a small button device.
In some cases, an additional procedure called a lateral tenodesis may be added to provide increased rotational stability and reduce the risk of graft re-rupture. This involves a small strip of tissue from the iliotibial band being re-routed around the outside of the knee.
Mr Gupté was involved in the research at Imperial College London from 2010 that helped develop this technique. Research shows it reduces re-rupture rates in certain patient groups, particularly those with hypermobility, excessive knee hyperextension, younger patients, and revision cases.
REHABILITATION
The Five Phases of ACL Recovery
ACL rehabilitation — whether surgical or non-surgical — progresses through five overlapping phases. Return to sport is based on functional criteria, not time alone.
‘Your ACL recovery is the runway to success. With or without surgery, rehabilitation helps get you airborne.’
YOUR SELF-CHECK: Can you stand on one leg for 10 seconds with your eyes closed? This simple test reflects neuromuscular control — the key target of ACL rehabilitation that is often overlooked in favour of strength alone. If you find it difficult, discuss proprioception training with your physiotherapist.
EVIDENCE BASE
What the Research Shows
REFERENCES — CLINICAL REFERENCES
- Frobell et al. (NEJM, 2010) — Early ACL reconstruction plus rehabilitation was not superior to rehabilitation alone with optional delayed surgery at 2 years.
- Grindem et al. (BJSM, 2016) — Functional criteria-based return to sport reduces re-injury rates significantly compared to time-based return.
- British Knee Society Guidelines (2022) — Shared decision-making recommended between patient and clinician when choosing between reconstruction and rehabilitation.
- Kittl C, El-Daou H, Athwal KK, Gupte CM, Weiler A, Williams A, Amis AA (2016) — The role of the anterolateral structures and the ACL in controlling laxity of the intact and ACL-deficient knee. American Journal of Sports
- Medicine 44(2):345–354. This Imperial College research, co-authored by Mr Gupté, provided the biomechanical rationale for lateral tenodesis by demonstrating that the iliotibial tract is the primary restraint of internal rotation at 30–90° flexion — not the anterolateral ligament as previously thought. Cited over 500 times globally.
- Kittl C, Halewood C, Stephen JM, Gupte CM, Weiler A, Williams A, Amis AA (2015) — Length change patterns in the lateral extra-articular structures of the knee and related reconstructions. American Journal of Sports Medicine 43(2):354–362. Defines the biomechanical basis for graft fixation angle in lateral tenodesis, directly informing how the modified Lemaire procedure is performed.
- Dodds AL, Halewood C, Gupte CM, Williams A, Amis AA (2014) — The anterolateral ligament: anatomy, length changes and association with the Segond fracture. Bone and Joint Journal 96-B:325–331. Co-authored research on the anatomy of the anterolateral structures that underpin the lateral tenodesis concept.
- Gompels B, Subramanian A, Gupte CM et al. (2026) — The Paediatric ACL National Audit (PANA) study: a multicentre review of UK practice and adherence to BOAST guidelines. The Knee. Led by Mr Gupté’s research group; sets national standards for paediatric ACL care.
- Khan A, Gupte CM (2024) — Paediatric Knee Injuries: A Narrative Review. British Journal of Hospital Medicine. Covers ACL and other knee injuries in children, including management principles.
- Pagliazzi G, Cuzzolin M, Pacchiarini L et al. (KSSTA, 2023) — Physeal-sparing ACL reconstruction provides better knee laxity restoration than transphyseal approaches in the paediatric population: a systematic review and meta-analysis of 49 studies, 3,260 patients. Physeal-sparing showed differential laxity of 0.22 mm vs 1.98 mm for complete transphyseal — and is the recommended approach in skeletally immature patients.
- Greiner JJ, Nazzal EM, Reddy RP, Hughes JD. In: Sherman et al. (eds.) Knee Arthroscopy and Knee Preservation Surgery (Springer, 2024) — Chapter on ACL anatomy and biomechanics. Confirms the ACL primarily resists anterior tibial translation AND provides rotatory stability through its two functional bundles; injury alters tibiofemoral contact points and increases meniscal strain. Ramp lesions of the posteromedial meniscus are present in up to 42% of ACL injuries and increase residual rotational laxity if untreated.