The medial and lateral collateral ligaments guide side-to-side motion and protect the knee from collapse. Most MCL injuries heal well without surgery. Understanding the grade and context of your injury guides the right treatment.
ANATOMY
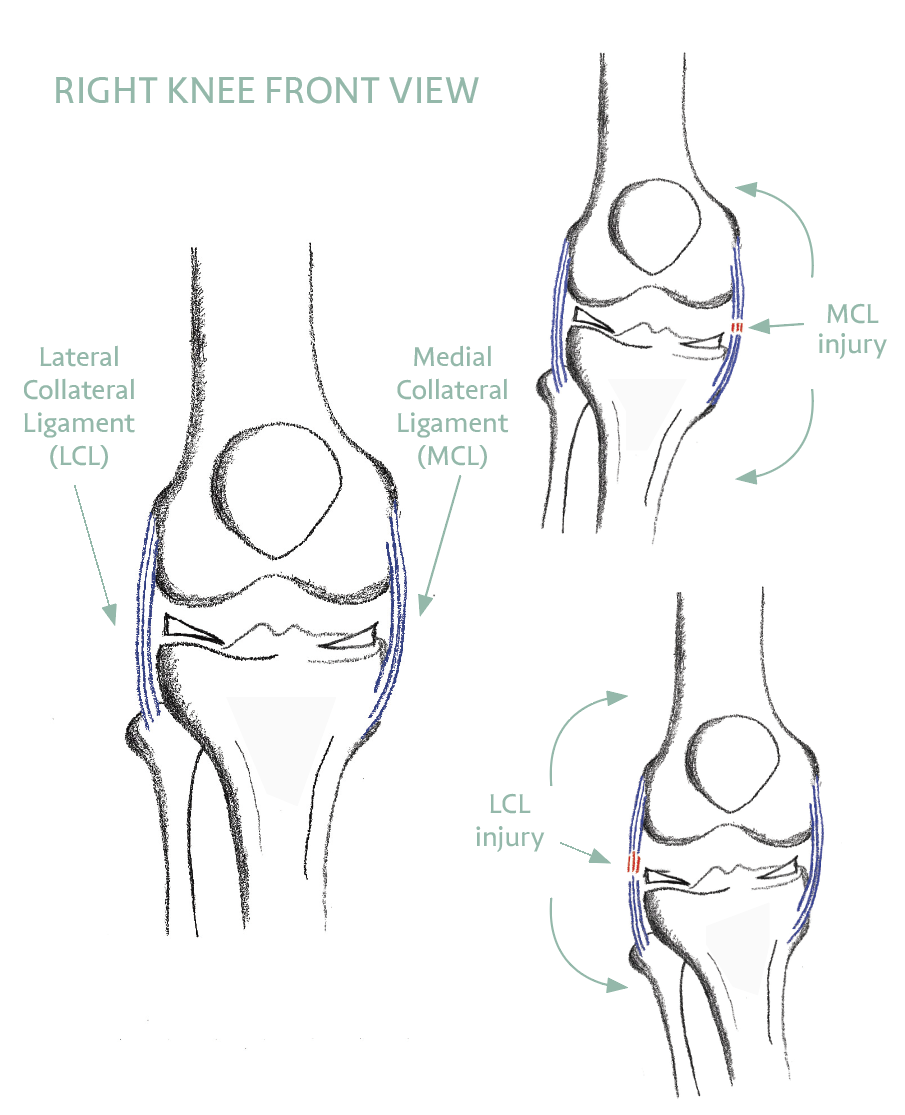
What the Collateral Ligaments Do
The medial collateral ligament (MCL) is a strong band of tissue connecting the femur to the tibia on the inner (medial) side of the knee. It provides stability against forces that push the knee inward — known as valgus forces — and is the most commonly injured knee ligament.
The lateral collateral ligament (LCL) runs along the outer side of the knee, connecting the femur to the fibula. It resists forces pushing the knee outward (varus forces). Isolated LCL injuries are less common, but the LCL can be injured as part of a more complex posterolateral corner injury.
A CLOSER LOOK
Layers, Partners, and Why It Heals
The MCL is not a single cord but two layers working together. The broad superficial layer is the largest structure on the inner side of the knee — roughly 10 to 12 cm long — and is the main restraint against the knee buckling inward. Beneath it, a deep layer blends with and anchors to the medial meniscus, which is why an injury on the inner side of the knee can sometimes involve the meniscus as well.
The MCL does not work alone. Just behind it, the posterior oblique ligament helps control rotation — particularly when the knee is straight. Clinicians describe these structures in terms of primary and secondary restraints: each direction of stress has one main stabiliser plus backups that share the load. The superficial MCL is the primary brake on inward (valgus) force while also providing secondary control of rotation — so even a significant MCL injury rarely leaves the knee without any protection.
There is also a biological reason MCL injuries heal so reliably. Unlike the cruciate ligaments deep inside the joint or the inner rim of the meniscus, the MCL has a generous blood supply — the genicular arteries run directly alongside and through it. Good blood flow delivers the cells and nutrients that repair tissue, which is why most MCL injuries, including many complete tears, mend well with time and rehabilitation rather than surgery.
On the outer side, the LCL is the primary restraint against the knee bowing outward. It rarely tears in isolation; when it does, it is often part of a wider posterolateral corner injury (Destination 9), which is why a careful assessment always looks beyond the ligament itself.