The posterolateral corner is a complex group of structures at the back and outer knee that controls rotation and overall stability. Injuries here are often subtle, frequently missed, and — if unrecognised — commonly cause failure of ACL or PCL reconstruction.
ANATOMY
What the PLC Does
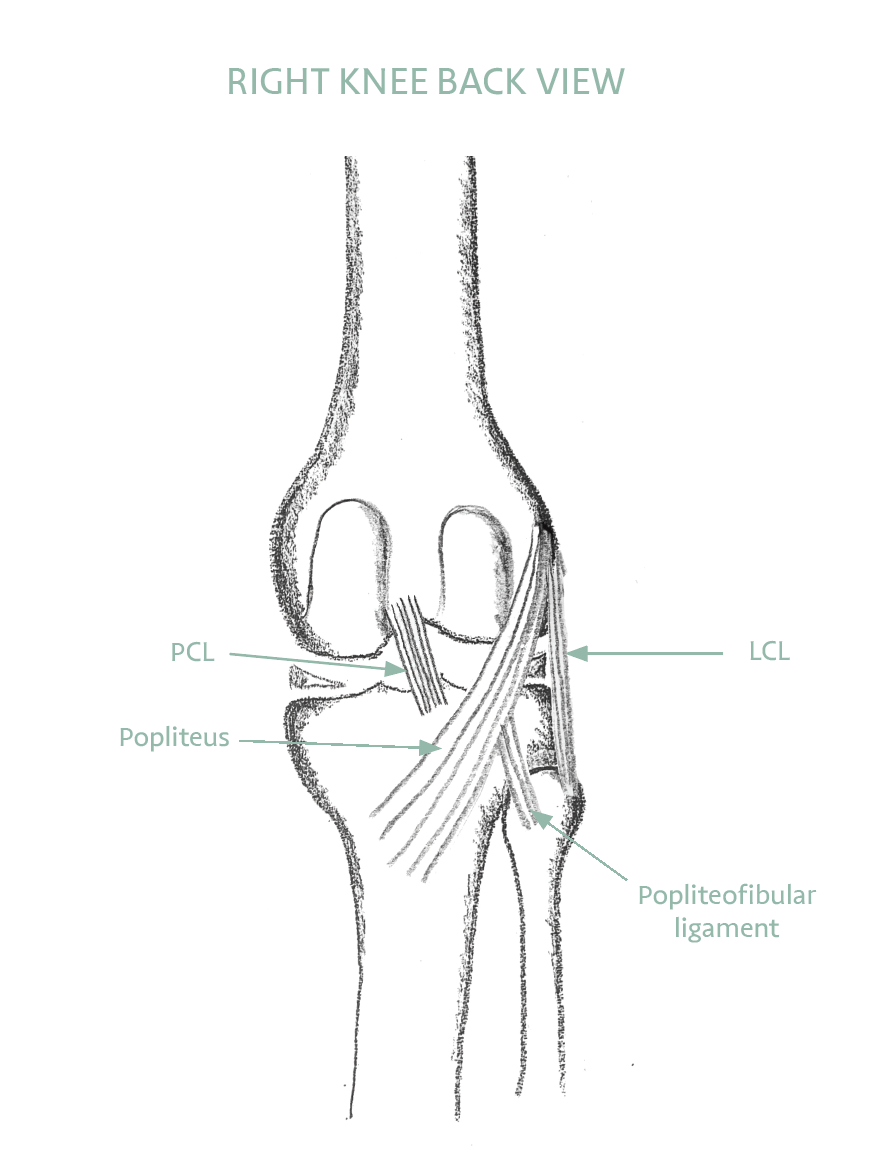
The posterolateral corner comprises several key structures: the lateral collateral ligament (LCL), the popliteus tendon, and the popliteofibular ligament, together with the posterior capsule and associated fibrous tissue. Working together, these resist external rotation of the tibia relative to the femur, and varus (outward bowing) forces on the knee.
This region was previously poorly understood and often referred to as the “dark side” of the knee — its anatomy was clarified largely through biomechanical research, including work from Mr Gupté’s group at Imperial College. A missed PLC injury is now recognised as one of the most common causes of ACL reconstruction failure.
HOW IT WORKS
Each Structure Has a Job
Although the posterolateral corner works as a unit, each structure has a defined role. The LCL is the primary restraint against the knee bowing outward. The popliteus tendon is the primary restraint against the shin rotating outward — the rotational control that gives this region its “guardian of rotation” name. The popliteofibular ligament backs both of them up, adding to rotational and outward-bowing control. Knowing which structure does what is what allows a surgeon to rebuild precisely what has been lost.
Because these structures are small, deep and overlapping, imaging alone can miss them — MRI is least reliable for the posterolateral corner, especially weeks or months after an injury. That is why a careful hands-on examination matters so much here. The dial test is the classic check: the clinician rotates the foot outward with the knee bent and compares the two sides. Extra outward rotation at 30 degrees of bend points to a posterolateral corner problem; extra rotation at both 30 and 90 degrees suggests the PCL is involved as well — another reason the corner and the PCL are always assessed together.
HOW PLC INJURIES HAPPEN
Mechanism and Associations
PLC injuries occur from direct varus force to the knee, hyperextension combined with varus stress, or high-energy trauma such as road accidents. They commonly occur alongside ACL or PCL tears in complex knee injuries. Isolated PLC injuries do occur but are less common.
The key clinical issue is that PLC injuries can be subtle — the initial examination may miss them, and the MRI interpretation requires specific knowledge of posterolateral anatomy. When a PLC injury co-exists with an ACL tear and is not identified, the persistent rotational instability will overload the ACL graft after reconstruction, leading to graft failure.
SIGNS OF PLC INJURY
- Outer (lateral) knee pain and tenderness
- A feeling of the knee giving way outward or into hyperextension
- Difficulty walking downhill or on uneven ground
- Instability during the stance phase of walking
- Associated ACL or PCL injury — always examine the PLC
- Abnormal external rotation on the dial test at 30° and/or 90°
‘It is especially important to detect PLC injuries when the ACL is also injured. A missed PLC injury is one of the most common causes of ACL graft failure.’