WHAT AFFECTS MOVEMENT QUALITY
The Factors That Control How Your Knee Moves
ACTIVE CONTROL
- Quadriceps — primary knee extensor and stabiliser
- Hamstrings — flex the knee and protect the ACL
- Hip abductors and glutes — control knee alignment
- Calf muscles — control foot and ankle position
- Nervous system — coordinates timing and force
PASSIVE RESTRAINTS
- ACL, PCL — sagittal plane stability
- MCL, LCL — coronal plane stability
- Posterolateral corner — rotational stability
- Menisci — load distribution and proprioception
- Joint capsule — limits end-range movement
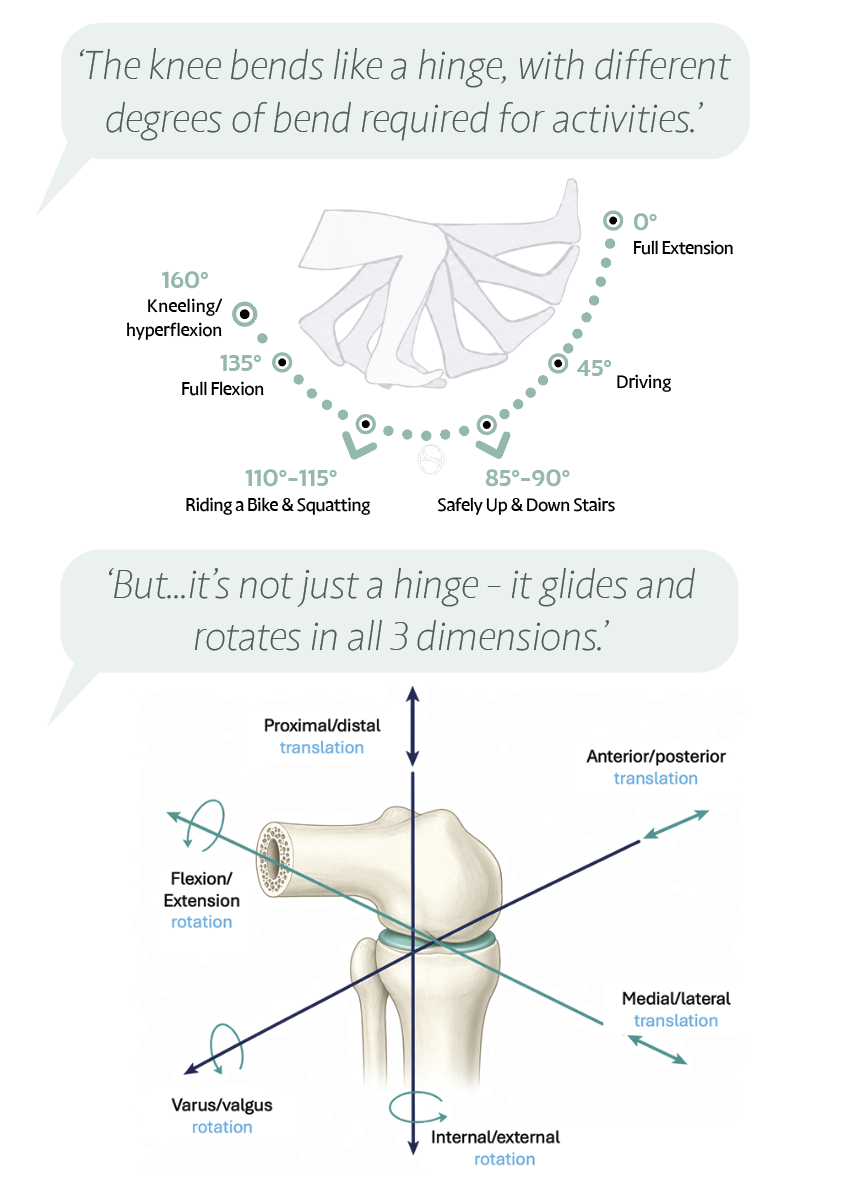
THE MECHANICS OF MOTION
How the Knee Locks and Unlocks
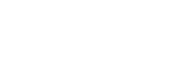
Roll and glide. The knee does not bend like a simple door hinge. As you flex, the rounded ends of the femur both roll and glide on the tibia, and the femur shifts gradually backwards — a movement called roll-back. This rearward shift is what creates the room for the knee to bend deeply, beyond a right angle, without the bones colliding.
Locking straight, unlocking to bend. In the last stretch of straightening, the tibia rotates slightly relative to the femur and the joint settles into a snug, stable position — the screw-home mechanism. This is why a fully straight knee feels solid and effortless to stand on: it is mechanically locked. To bend again, the knee must first quietly unlock. The process is automatic and you never notice it, but it is central to how the knee carries you with so little muscular effort when you stand.
A pivot on the inside. The two sides of the knee do not move identically. The inner (medial) side glides more and acts as a relatively stable pivot, while the outer (lateral) side rolls and travels further. The result is a small, natural rotation built into every bend and straighten — the knee turning gently around its inner edge.
One link in a chain. The knee never works alone. It sits in the middle of a chain that runs from the spine through the hip and down to the ankle, and the segments above and below strongly influence it. Weakness or stiffness at the hip or ankle changes the demands on the knee — which is exactly why good rehabilitation looks beyond the knee itself to the glutes, hips and calves.
Control can be trained. Reassuringly, the knee’s stability is not fixed by anatomy alone. Coordinated muscle timing and reflexes can compensate for a great deal, and targeted neuromuscular training has been shown to help the joint move with more stability and confidence — even where the passive structures are doing less of the work.
‘Think of straightening your knee fully as clicking it into a locked, restful position — and bending as gently unlocking it again. Trusting that lock is part of moving with confidence.’
YOUR SELF-CHECK: After sitting for an hour, stand up and take 10 slow steps. Does your knee improve after those first steps? That warming-up process is the synovial fluid distributing through the joint. If it does not improve, speak to your clinician.
REFERENCES — CLINICAL REFERENCES
- Dye SF (2005) — The knee as a biologic transmission: the envelope of function concept. Clinical Orthopaedics and Related Research.
- Gupte CM et al. (Journal of Biomechanics, 2002) — A new technique for measuring the screw-home movement of the knee: results in normal knees and knees after transection of the ACL.
- Reynolds RJ, Michelet A, Müller JH, Saffarini M (2022) — Kinematics of the Native Knee. In: Becker, Hirschmann & Kort (eds.), Basics in Primary Knee Arthroplasty. Springer.